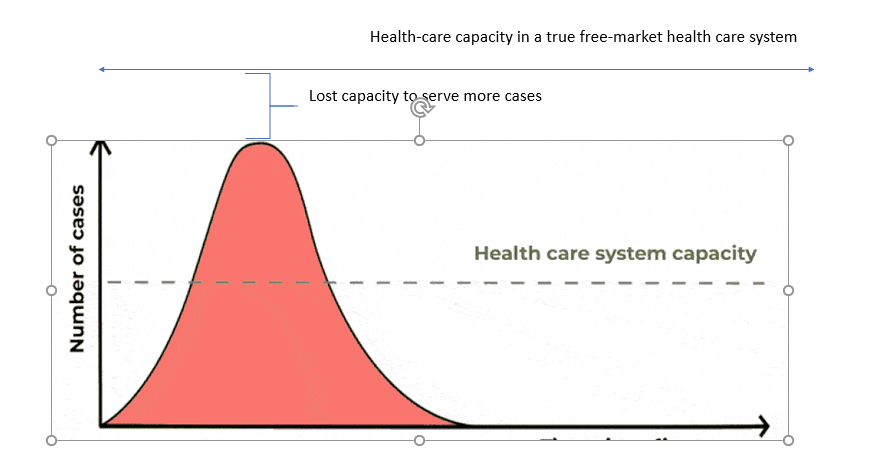
With the coronavirus we have heard time and time again of the flattening of the curve. The basic premise is that we have to stretch out the number of cases of coronavirus due to the restraints within the healthcare system. There is some truth to this given any system can only absorb so much demand in a finite period of time (there aren't endless resources after all). However, what gets missed in this view is the opportunity of the unseen as so many regulations and red tape prevents the expansion of the capacity for healthcare services.
The first thing to understand is how the government (mainly the CDC/FDA) totally mismanaged the testing for coronavirus. As I detail in my last post detailing how the CDC created it's own faulty test and then the FDA required the CDC to retest every positive coronavirus test for accuracy. If you remember in the early days of coronavirus anyone who tested positive for coronavirus "had" to have their sample sent to the CDC center in Atlanta. Even scientists in Seattle who tried to run their own testing were shut down by the CDC and FDA (their lab wasn't up to Medicare standards). In my last post I detailed the massive amount of regulation regarding lab testing (The Clinical Improvement Act of 1967 plays a large role in this). Also the FDA was asking this Seattle lab to require any of their samples to be run 5 times for accuracy (also this is utterly impractical given at the time there were few cases of coronavirus). Now you sit back and say to yourself how many people have gone un-diagnosed/passed away because of the mismanagement from the FDA and CDC? The FDA/CDC should have immediately let private companies and organizations testing organizations come on the scene to rapidly implement the tests they already have. If this had happened you would have seen tests been quickly deployed and individuals learning whether or not they had the virus so they could have determined whether or not to isolate themselves. Fortunately the FDA has backed down on the regulation front and currently 80 different companies are trying to apply to develop testing. You have companies that are innovating at home tests, blood tests that take 8-10 minutes, and developing processes for testing that the CDC/FDA would never dream of.
There have been talks the United States will run out of hospital beds to care for coronavirus patients. Looking at the data the United States is a little over 6,100 hospitals in the United States (this includes profit and not for profit hospitals). This translates into roughly 924,000 beds that can be used at any given time. However, at any given time roughly 66% of hospital beds are full. Running the quick math this would say that there are roughly a little over 300,000 hospital beds available. If you look back to 1975 there were actually more hospital beds then there are today (back then close to 1.5 million beds and there were also only 216 million people in the country at that time vs. 330 million people today. To translate this number this would say in 1975 we had a hospital bed for .69% of the US population vs. 28% today. Now it should be pointed out that there have been advancements made in medicine that has reduced the need for people to not require hospitalization. Another way to look at the number of hospital beds is per 1,000. The United States has 2.8 beds/1,000 people. Actually this is similar to Italy (3.2 bed/1000 people) and greatly lagging behind South Korea with 12 beds/1,000 people. Moving towards a country with more hospital beds would be a wise decision. However, the regulatory burden to open a hospital doesn't allow just anyone to open a hospital.
I haven't seen anyone study the regulation of hospitals but I did some research regarding what would it take to open up a hospital (this blog gets into the details). Well first you have to get a license from the state (I found the one for Texas which is 14 pages here). Also you shouldn't forget your fire safety report too. Also before you even get state the occupancy of your hospital you have to get approval by the Architectural Review Group of Health and Human Services. The Architectural Review Group has to approve an application before any construction begins (this is about 9 different steps by itself). It is also recommended for the applicant of the hospital to attend a feasibility conference before they get approval. Once all that is approved you will have to pay a license fee of $39/bed (which is not refundable). Then if you want to get certified by the Joint Commission that will run you about $46,000 per year. If you plan to get any type of funding from Medicare you will have to at least abide by these rules. Clearly, opening a hospital is time and capital intensive and has large barriers to entry. I haven't even gotten into the certificate of need (CON) laws that allow existing hospitals/medical facilities to block the opening of hospitals that are considering opening which reduces the number of potential hospital beds by tens of thousands.
On the other hand you have innovators like Dr. Devi Shetty who is able to open up hospitals all around the world and a hospital was built at a cost of $700,000 per bed (a 65% discount) to the $2 million per bed it would cost in the United States. These hospitals also negotiate prices with their suppliers. For example when the hospital was looking at disposable gowns one company offered to make the gowns for $75 and the hospital found a factory that could make the gowns for $37. If hospitals in the United States operated liked this not only would the cost of healthcare drop but the quality would increase as well as there would be more competition.
For years I have been saying for roughly the past decade that the FDA has over regulated and has left individuals with fewer options (to treat their own life). If the FDA simply had a longer Phase I trial to just simply test the safety of a drug and report the results and allow patients and healthcare professionals to determine what is best for them (also it is important to note the prices of drugs would decrease as there would be more competition). What people seem to forget is it takes a drug company roughly $2.5 billion of capital and 12 years to bring a drug to market to patients. If you just say the average life expectancy of the America is 78 years you have to wait 13% of your lifetime to watch one new drug get approved. The chances of getting a drug from the molecule level to market is 1 in 5,000. Now the important question to ask is how many drugs that were submitted to the FDA were safe however not approved for whatever reason (the FDA seems to believe we all comprise of the same biology-even though this is utterly insane). On the one plus side Mr. Kevan Shokat (chemist at UCSF is sifting through 20,000 drugs approved by the FDA to see if there are possible drug candidates for coronavirus. Now if the FDA just stuck to approving drugs that were safe that database could be have a multiple of the number of drugs approved today and possibly alleviate some of the symptoms from the coronavirus. Also it is important to consider once a drug is approved it is only approved for one use (cancer, heart issue, etc.). However, the reality is some drugs are used to treat multiple things (example Propecia was used originally used to treat men who had an enlarged prostate but then was found to help men regrow their hair). However, the FDA will not allow companies to tout additional benefits other than what the drug was originally approved for. Once a drug is approved however the FDA can't limit or control how drugs are prescribed. Doctors and patients should be allowed (once a drug is approved) to use that drug in anyway they see fit. Often times the doctor is knowledgeable about the patient's medical history/previous experience with drugs taken/aware of the benefits and side effects of the drug. Also let's not forget patients these days are armed with information too and often times are just as up to speed as doctors for treatments (especially if they have a chronic illness). It is worth noting too that there are specific databases for off-label use were medical providers compare notes on the drugs used, how effective they are, case studies, dosing issues, and the risk/benefit considerations when factoring in whether or not to prescribe certain drugs. The Wolters Kluwer database has over 2400 off-label uses. Allowing researchers/doctors to try different drugs for off-label use may potentially find a treatment to alleviate some of the symptoms of coronavirus.
While we are on the topic of drugs it is important to point out the number of drug shortages. The University of Utah actually keeps track of the drugs that currently have a shortage. As I write this roughly 207 drugs are on the list. Roughly close to 50 drugs have been added to the list within the last week. Again the reason for the drug shortages has to do with the over-burdensome regulation of the FDA. If you have half a day to kill you can read through some of the regulations here. The regulations focus on things like the type of equipment used, the water quality used to make the drugs, how often your facility has been inspected, the records kept by the lab, packaging and labeling, along with personnel requirements. The FDA in recent years has increased their regulation of manufacturers and have adopted a "zero tolerance policy". Drug manufacturers must ask the FDA for approval to make the drug, then get approval on how much of the drug it plans to make, and agree on the time frame. Also if a one drug manufacturer shuts down another drug manufacturer can't increase it's production without FDA approval. Also a program as the 340B drug rebate program allows hospitals and clinics to get discounts (between 13-23%) on drugs in order to provide these drugs to provide to patients on Medicaid (low-income) which then allows these medical institutions that participate in the program to stockpile drugs at a reduced cost. Drug shortages will continue to grow in this time of crisis and not allow patients to truly receive the treatments they need unless the FDA reverses course lightening the regulation and become more flexible in allowing companies to produce the drugs that some people are in desperate need of.
Also some other low hanging fruit is to reduce the regulatory burden on physician assistants/nurse practitioners. Currently 29 states require some level of supervision for nurse practitioners and 20 states require a percentage of physician assistant charts to be co-signed by the physician. There are more than 290,000 nurse practitioners and 118,000 physician assistants. If regulations in these professions were relaxed doctors, physicians assistants, and regular physicians would save tens of thousands of hours that could be used to treat patients who are suffering from coronavirus.
In this time of crisis however there are some creative solutions. For instance empty hotel rooms are being turned into hospitals and even using cruise ships for additional hotel rooms. Speaking of other sensible regulations that allow individuals who may have an out of state medical license to practice in different states. Even Medicare has expanded to include telemedicine (it is important to note that private companies have been using medicine for years.
Instead of flattening the curve the focus should be expanding the curve by reducing regulation to allow more drugs, procedures, medical professional and resources to work on the problem. If the FDA and CDC had allowed more testing companies to get their product out to the market more people would have known whether or not they had the coronavirus and then the public would have better information has to who should stay home or who is okay to go out (instead many states have shut down for business). The lack of the number of hospital beds could be greatly helped by reducing the barriers to entry. We need more innovation in terms of letting more companies and individuals open more hospitals that could be housing coronavirus patients. Letting the FDA relax their rules regarding off-label use would work wonders to allow researchers to experiment with any drug that is approved by the FDA may help find some accidental wonder drug that could help. While we are on the topic of the FDA having them back down on the "zero tolerance" for drug manufacturers would reduce the number of drug shortages which is critical in times like this were patients need these drugs the most. Lastly, allowing states to not require nurse practitioners to be supervised or require physician assistants to have their charts co signed by doctors would free up the much needed time of medical professionals to attend to sickly patients who are in need of treatment (and also reduce the work load on these medical professionals who are already burning out). Attacking all of these issues would help not only expand the curve of possibilities but end of saving more lives, improve the quality of living, and reduce the red tape for researchers, doctors, and medical practitioners and result in a win-win for everyone.






No comments:
Post a Comment